
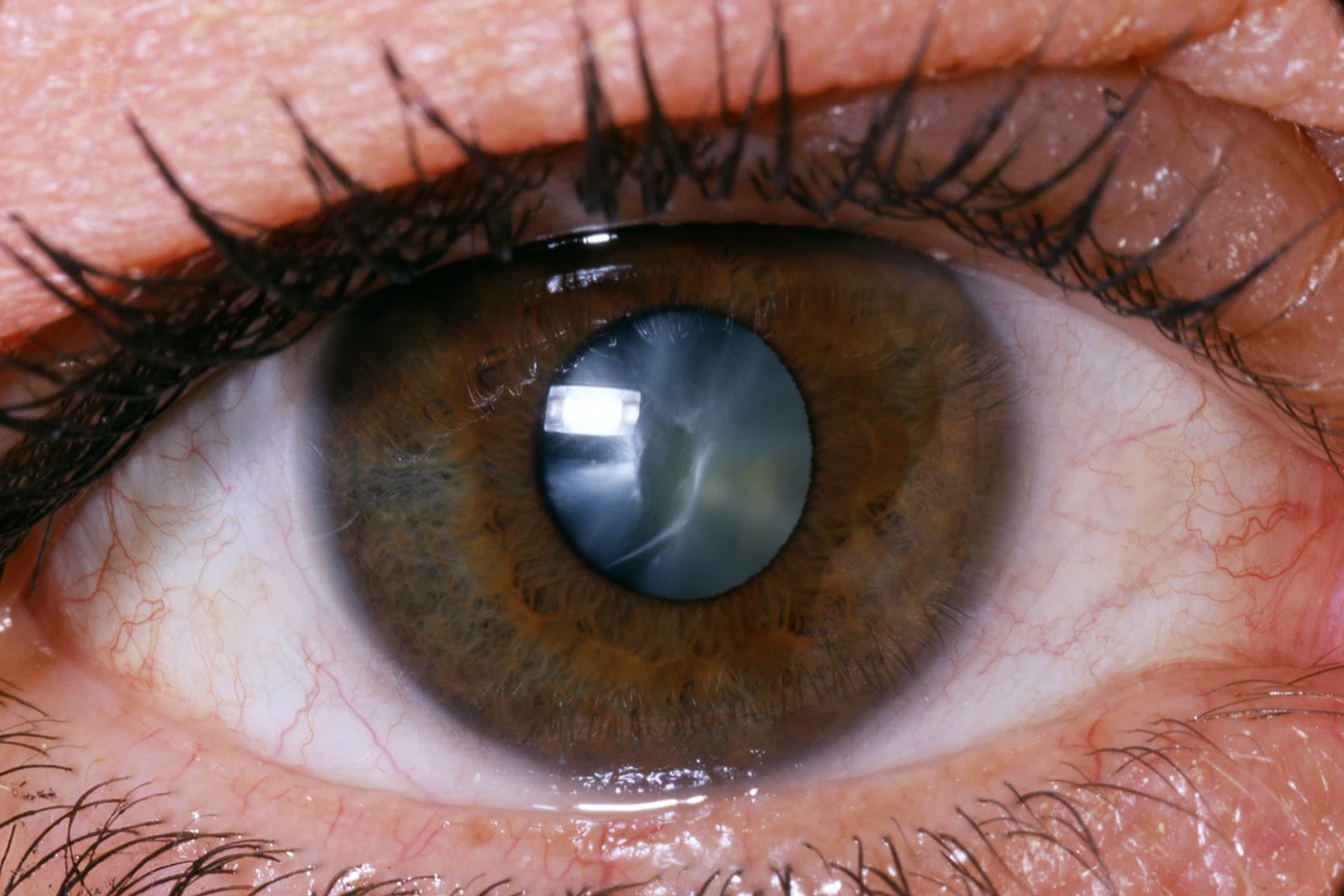
Preventing and managing vitreous loss after cataract surgery
Vitreous loss is connected with a poor visual result following cataract surgery. Vitreous loss is less common among experienced surgeons and those who undertake a significant volume of cataract surgeries.…
